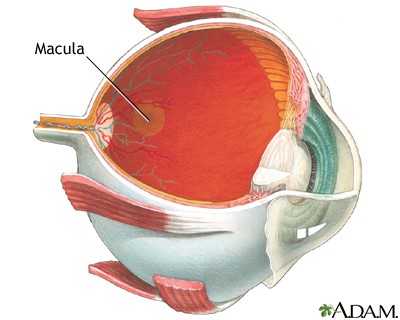
To understand age-related macular degeneration (AMD), the most common cause of legal blindness in older people, you need to understand the macula. First, think of the eye as a hollow globe made of three layers. The white, outside layer is the sclera. Inside the sclera is a middle layer called the choroid, which contains networks of tiny blood vessels called capillaries. The inner layer, called the retina, contains pigment-filled cells that absorb light, light receptor cells call rods and cones that change light into electrical information, and nerve cells that transmit that information to the brain. In the center of the retina, there is a tiny yellow spot about the diameter of a pencil eraser called the macula lutea (Latin for yellow spot).
What does the macula do? Try looking at a star to find out.
The macula contains only cone receptors, which detect color, and is responsible for sharply focused vision. If the macula degenerates, visual clarity is lost. The other 96% of the retina contains mostly rods, non-color receptors that perceive dim light and movement and are responsible for peripheral vision. When you look at stars, you see them only with your peripheral vision. Trying to focus on a single star makes it disappear because the macular cones require more light than the night sky offers. Imagine the disappearance of anything you try to focus on, in any kind of light, and you have some grasp of what macular degeneration is like.
When the macula degenerates
Age-related macular degeneration moves slowly, with many years between the first visible changes in the retina and the onset of symptoms. The first symptoms come from decreasing visual sharpness. Reading speed declines. Reading glasses no longer work for fine print. Road signs look blurred. With progression, dark patches or blank spots appear when patients focus on faces or print, and sometimes straight lines appear wavy. Legal blindness (best corrected vision less than 20/200) comes later and is never total because peripheral vision is spared, even though some of the same degenerative changes affect other parts of the retina. The macula is simply so tiny and so specialized that small areas of damage interfere with the ability to see clearly.
What’s the cause of macular degeneration?
No one knows for certain what causes macular degeneration but ophthalmologists suspect that the vascular anatomy of the retina plays a significant role. While the macula looks yellow, the rest of the retina has a reddish hue because of an overlying bed of capillaries, branches of the retinal arteries and veins which spread like a tree over the retinal surface. The tree stops at the macula and this vital region depends solely on blood flow through the network of tiny capillaries in the choroid layer for oxygen and nutrients and for clearing away the products of its high rate of energy use. The first changes that signal possible AMD, visible long before any symptoms appear, occur in the microscopic space between the choroid layer and the retina and are called Drüsen.
Signs of deterioration
Drüsen are yellowish accumulations of fats and proteins and inflammatory substances. Small, sharper edged patches called hard drüsen are commonly seen in other parts of the retina and do not interfere with vision, but larger, fluffy patches, especially in the area of the macula warrant more frequent follow-up exams because people who have them sometimes, but not always, develop symptoms of AMD. If visual symptoms occur and drüsen are present, the diagnosis is dry macular degeneration. In about 10-20% of cases of dry macular degeneration, new tiny blood vessels poke through to the retinal layer from the choroid, a process called neovascularization. When this happens, the diagnosis becomes wet macular degeneration which reflects the tendency of these blood vessels to leak and bleed, causing more cell destruction and separation of the retina form its underlying supporting layers.
Who’s at risk for macular degeneration?
The primary risk factors for macular degeneration are age, smoking and increased body mass index. A family history of macular degeneration also increases the chances of its occurrence, but so many different genes are involved that predictive genetic testing is not useful. Diabetes and vascular disease can accelerate the degenerative process. On the positive side, diets rich in green leafy vegetables, particularly those containing abundant antioxidants called carotenoids, as well as diets rich in Vitamins C and E, and those rich in zinc have been associated with lower frequencies of macular degeneration.
Other eye problems are more common
Fortunately, AMD is much less common than other age-related visual problems like presbyopia (poor near vision) and cataracts, both of which are eminently treatable. AMD affects about 2% of people in their 70s. Prevalence jumps to about 14% in Caucasians who reach their 90s, but remains at about 2% in other races. Legal blindness typically does not occur until the eighties.
Treatment
There is no treatment for dry macular degeneration. The positive correlation between dietary antioxidant consumption and lower rates of AMD has led to the development of the “eye vitamins,” and while studies have shown some slowing of the degenerative process when these vitamins are consumed, there is no evidence that taking them prevents the onset of the disease.
The first line of treatment for wet macular degeneration is injection, directly into the eye, of drugs which block new blood vessel formation. This slows the disease process, but does not cure it. Another treatment is photocoagulation, or the injection of drugs which, once activated by light aimed at the new blood vessels causes them to shrivel. Laser treatment of troublesome blood vessels is commonly done, but it destroys the retina in the area treated, so its aim is prevention of new problems. Surgery is sometimes required to drain fluid accumulations or reattach retinal tears.
Preliminary studies suggest that high dose cholesterol lowering drugs (statins) may shrink drüsen, but one worrisome study of data from a large managed care group suggested that statin use for over a year increased rates of progression of dry AMD to wet AMD. Long term prospective studies are needed, and eye exams should be routine for anyone taking statins.
Useful Macular Degeneration websites
https://nei.nih.gov/health/maculardegen/armd_facts
