Episodes of back pain and stiffness are common and often begin young adulthood. Some, but by no means all, presage a lifetime of back trouble. The saga of President John F. Kennedy’s chronic back pain began during his college years at Harvard, entailed several failed surgical procedures during his early political career, and, according to some armchair medical detectives, may have contributed to his death in Dallas in 1963, when the rigid back brace which he wore kept him in an upright position after the first shot hit him, positioning him for the lethal head shot. Medical sleuths have also combed his medical records in an attempt to understand the origin of the back pain which became his everyday companion in his post college years. As with many back pain sufferers, the beginnings of JFK’s pain complaints had no clear relationship to a single injury, and were not accompanied by visible X-ray abnormalities. So what is the mechanism of this type of pain? What does it mean when someone’s back “locks up,” for days at a time, both in the moment and as an indicator of future problems?
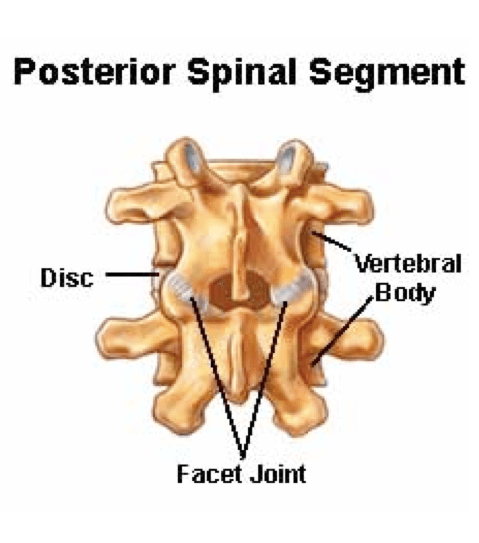
Episodes of stiffness and back pain in the lumbar region are almost always related to the moving parts of the spine, of which there are two types – the cushioning discs between the vertebral bodies, and the facet joints of the bony arches that emerge from the back of the vertebral bone and surround the spinal cord and nerve roots. Facet joints are the pairs of bony surfaces that match one vertebral body’s arch with the ones above and below it in the column of spinal bones (see image below). The surfaces of these tiny joints are covered with cartilage and bathed in synovial fluid, just like large joints. Each facet joints is wrapped in connective tissue which stretches to allow movement. The construction of the facet joint allows a lot of forward flexion, a small amount of backward extension, and protects against too much rotation, which might cause disc movement.
Very often, low back stiffness begins after a night in bed, on the day after an unusually lengthy activity involving bending, lifting, running, biking, or even walking. Imagine a bit of swelling and inflammation in the connective tissue surrounding a facet joint, causing irritation of its rich supply of tiny nerves. The mission of these nerves is protective, to shriek warnings when you pull a joint too far out of line. When they are bathed in inflammatory cytokines after a bout of overstretching, they speak with varying degrees of urgency to stop you from moving those joints any more until the healing processes have time to clean up the damage. They engage reflexive muscle contraction to do the work of preventing motion, giving you the sense that the back has locked itself into one position. When this happens you suddenly appreciates how much flexibility your low back has under normal circumstances.
A good history and physical examination is usually sufficient to pin blame on the facet joints. Pain is generally confined to the mid and low back, but can radiate more widely because pain signals spread out along neighboring pathways. It is worse in the morning or after prolonged sitting, and can be worsened by some motions like twisting or bending backwards. Bending forward often improves the symptoms. Muscles are palpably tense and sometimes tender. If there are no physical signs of pressure on spinal nerves, and if there is no history of a fall or blow, imaging studies are not necessary unless conservative treatments over the next few weeks fail. At times, particularly if the pain is one-sided, injection of the suspected problem joint with an anesthetic helps pinpoint the diagnosis by temporarily relieving the pain.
Ice application is often helpful early on, but over the course of the next few days heat packs may be better since they increase blood flow and help healing. Anti-inflammatory drugs can ease the pain. Gentle aerobic activity counteracts the tendency of the back to stiffen more with prolonged sitting or lying. In most cases, the pain will run its course in a week to 10 days. A good physical therapist can help with massage or ultrasound treatments, passive stretching and exercise recommendations.
While most episodes of the back “locking up” are self-limited and not accompanied by structural problems such as disc herniations or bony overgrowth, the pain is an early warning system indicating that the back is being asked to perform under some strain it can not tolerate. Beyond the acute phase, a physical therapist can help interpret the message the painful episode was delivering. What set you up for the painful response? The facet joints seldom get irritated in childhood unless there is an underlying orthopedic anomaly or asymmetry. But by the time of young adulthood, chronic postural problems may be blooming. Most shoes are guilty of tipping the upright body forward because most shoes, even ergonomic running shoes, have heel elevations of at least an inch. Hamstring muscles become tighter and abdominal muscles weaker. Excess body weight and too much sitting hunched over a keyboard may be taking a toll. Overworked facet joints may not complain much until they are subjected to an unusual amount of activity, but when they do it is time to try to relieve them of daily irritants and extra work to avoid recurrence of the painful bout and degeneration of the bony structures.
JFK’s back history is instructive because, while he began with back pain episodes of a somewhat vague nature and had normal bone structure, he suffered through three failed back surgeries, a terrible postoperative wound infection, and hundreds of injections of anesthetics into his back joints. Eventually he got to a conservative physical therapy approach (the White House swimming pool is its legacy), and for a time was more comfortable. Had this been the earliest line of therapy perhaps he might not have been wearing that rigid back brace in Dallas.